Author: Mary Jefferson, RDN, LD, MS, CDCES
For women living with Type 1 Diabetes (T1D), navigating blood sugar management is a daily science experiment. Often, seemingly healthy choices—like adding whole milk The Hook: You weighed the oats. You measured the honey. You calculated the exact insulin-to-carb ratio for your morning bowl of oatmeal and whole milk. Yet, two hours later, your continuous glucose monitor (CGM) is alarming with a stubborn, unexplained spike. The math was flawless. So, what failed?
The answer isn’t a miscalculation. It is a fundamental shift in the baseline metabolic environment. When standard carbohydrate counting fails to explain postprandial hyperglycemia, it is time to examine the powerful intersection of dietary biochemistry and the endocrine system.
Let’s break down exactly what happens when high-demand macronutrients collide with cyclical hormones.
The Dietary Variables: Beyond Carbohydrates
Before looking at the cycle, we have to look at the bowl. Whole milk and oatmeal present a complex metabolic challenge for individuals managing Type 1 Diabetes (T1D).
- The Glucagon Trigger: Dairy is highly “insulinogenic,” meaning its Food Insulin Index (FII) exceeds its carbohydrate footprint. The whey protein in milk is dense in branched-chain amino acids (BCAAs). These BCAAs trigger the rapid release of glucagon, signaling the liver to dump endogenous stored glucose into the bloodstream.
- The Lipid Load: Full-fat dairy introduces a heavy lipid load that delays gastric emptying. As the body processes these fats, circulating free fatty acids induce acute insulin resistance, stretching the digestion of the oats and honey over several hours.
To see how these variables play out in real-time, we have to look at the hormonal landscape at the time of consumption.
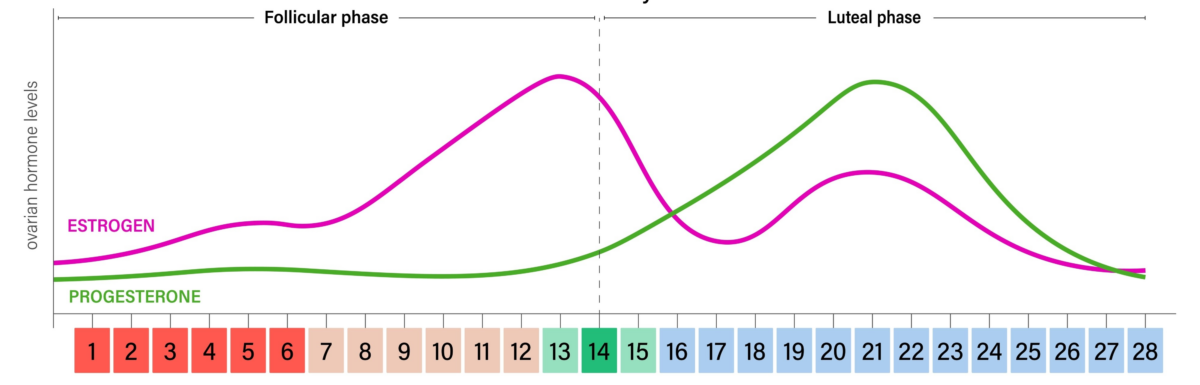
Scenario A: The Follicular Phase (Days 1–14)
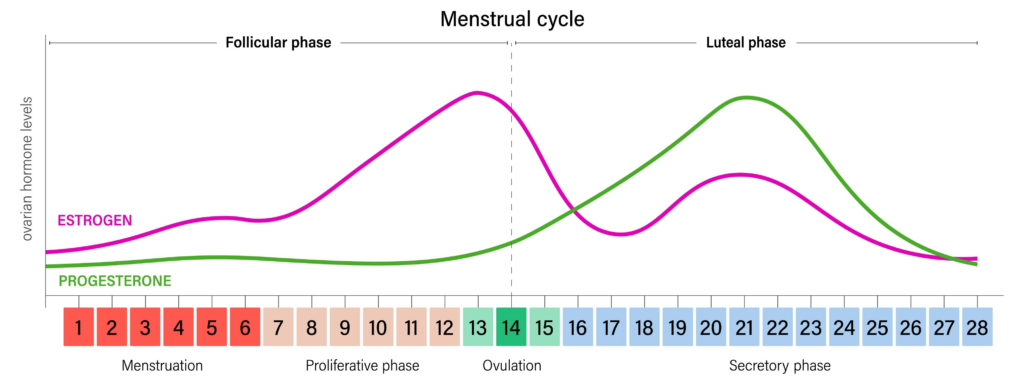
The metabolic environment: High Insulin Sensitivity.
Starting on day one of menstruation and peaking right before ovulation, estrogen (estradiol) dominates. Estrogen is highly insulin-sensitizing. It upregulates the expression of GLUT4 transporters. The cellular doors are primed to pull glucose out of the blood.
The Biochemical Reaction:
- The Input: The oats and honey deliver a rapid glucose load.
- The Trigger: The whey protein BCAAs trigger a glucagon surge and subsequent endogenous glucose release.
- The Clearance: Because estrogen has highly sensitized the cells, the exogenous insulin bolus binds efficiently to the receptors. The GLUT4 transporters open rapidly, clearing both the dietary glucose and the hepatic glucose dump. The standard insulin-to-carb ratio successfully manages the delayed lipid load. Blood glucose remains stable.
Scenario B: The Luteal Phase (Days 21–28)
The metabolic environment: Peak Insulin Resistance.
Following ovulation, progesterone takes over. Progesterone is inherently insulin-antagonistic, biologically designed to keep glucose circulating in the blood. At the cellular level, it degrades Insulin Receptor Substrate-1 (IRS-1) and inhibits the PI3K signaling pathway.
The Biochemical Reaction:
- The Blockade: Progesterone has effectively locked the cell. Even when the injected insulin binds to the surface receptors, the internal PI3K signaling is blocked. The GLUT4 doors stay shut.
- The Surge: The whey protein triggers the liver to dump endogenous glucose into an already elevated bloodstream.
- The Traffic Jam: The lipids from the whole milk flood the bloodstream with free fatty acids, extending the state of acute insulin resistance.
- The Result: A metabolic perfect storm. The glucose from the oats, the glucose from the liver, and the delayed digestion from the fat all crash into cells that are locked down by progesterone. Baseline insulin requirements predictably jump by 20% to 40%, rendering standard bolus calculations ineffective and resulting in prolonged hyperglycemia.
The Clinical Strategy: Cycle Syncing
Glycemic variability during the luteal phase is a measurable biological equation. Standard carbohydrate counting alone is insufficient when dealing with high-glycemic carbohydrates combined with high-FII proteins and delayed-digestion fats.
The Action Plan: By tracking menstrual cycle data alongside a CGM, the specific luteal phase resistance window (typically Days 21–28) can be mapped.
Implementing a secondary Luteal Basal Profile on an insulin pump—preemptively increasing baseline delivery by 20% to 40% during this timeframe—addresses the progesterone-induced resistance before the meal even begins. Anticipating these endocrine shifts allows for better, proactive blood sugar management, transforming unpredictable spikes into a much more manageable, predictable pattern.
Citations and References
- Holt, S. H., Miller, J. C., & Petocz, P. (1997). An insulin index of foods: the insulin demand generated by 1000-kJ portions of common foods. The American Journal of Clinical Nutrition, 66(5), 1264-1276.
- Bao, J., Atkinson, F., Petocz, P., Willett, W. C., & Brand-Miller, J. C. (2011). Prediction of postprandial glycemia and insulinemia in lean, young, healthy adults: glycemic load compared with carbohydrate content alone. The American Journal of Clinical Nutrition, 93(5), 984-996.
- Brown, S. A., Jiang, B., McElwee-Malloy, M., Wakeman, C., & Breton, M. D. (2015). Fluctuations of hyperglycemia and insulin sensitivity are linked to menstrual cycle phases in women with Type 1 diabetes. Journal of Diabetes Science and Technology, 9(6), 1192-1199.
- Yeung, E. H., Zhang, C., Albert, P. S., Mumford, S. L., Ye, A., Perkins, N. J., … & Schisterman, E. F. (2010). Adiposity and sex hormones across the menstrual cycle: the BioCycle Study. International Journal of Obesity, 37(2), 237-243.

About Mary Jefferson, RDN, MD, LD, CDCES
Diagnosed with type 1 diabetes more than 30 years ago, Mary K. Jefferson brings both professional expertise and lived experience to every client relationship. She specializes in insulin and medication management, weight management, Intuitive Eating, carbohydrate counting, and advanced insulin pump strategies, helping individuals create personalized and sustainable approaches to diabetes care that fit real life — not perfection.
Mary previously practiced at Intermountain Healthcare in Salt Lake City, where she supported people across a wide range of diabetes needs and stages of life. Her approach combines clinical knowledge with compassion, practicality, and deep understanding of the everyday challenges that come with managing diabetes.
Known for her warm and supportive style, Mary is passionate about helping people feel more confident, less overwhelmed, and more empowered in their care. She believes diabetes management should improve quality of life — not take it over — and works closely with each person to build strategies that support both physical health and emotional well-being.